Tools and resources
The following tools and trainings can help improve health equity outcomes.
Health equity tools
The Ontario Ministry of Health and Long-term Care (2012) developed the HEIA tool to improve health equity and reduce disparities in health outcomes between population groups. The HEIA is a decision support tool that includes a series of steps to help leaders and program planners identify how a program, policy or similar initiative will impact population groups in different ways. It also identifies unintended potential impacts.
The University of Victoria’s Equity Lens in Public Health project created an inventory of health equity tools:
The following document provides detailed descriptions of each tool including the objective, intended users, how the tool can be used, and any information available about application and evaluation of the tool.
Access Alliance Multicultural Health and Community Services and the Alliance for Healthier Communities created this toolkit, which maps the resources that are available to build capacity around health equity, at the individual, team, and organizational levels. It represents a compilation of all the tools and resources created and gathered throughout the project to create the toolkit.
Anti-racism tools and strategies
It is important to touch on anti-Black racism because “history requires us to recognize Black experiences with racism as uniquely different from other experiences with racism.” (CAMH, 2021a, p. 8)
Anti-Black racism is a systemic form of prejudice, discrimination or antagonism that intentionally or unintentionally harms people of African and Caribbean origin through systems and structures that exclude, silence, devalue and marginalize Black experiences. Anti-Black racism is rooted in the history and legacies of slavery and colonization. It continues to uphold narratives of white superiority and Black inferiority, thereby creating and reproducing prejudices, stereotypes and disadvantages for Black people (Black Health Alliance, n.d.).
Black people of African and Caribbean descent are not a homogenous group. There are differences in generation status, ethnic and cultural origin, immigration, geography, language and more (CAMH, 2021b). These differences mean that one size does not fit all when delivering programs and services.
The Centre for Addiction and Mental Health and the Anti-Black Racism and Mental Health Advisory Committee created the Dismantling Anti-Black Racism Strategy. It identifies key priority areas at the organizational, staff and clinical level, and includes 22 actions that aim to decrease anti-Black racism at CAMH.
Project Implicit, delivered from Harvard University, is a non-profit organization and international collaborative of researchers who are interested in implicit social cognition. Its “implicit association test” allows you to assess your unconscious bias.
The Peel CAS has outlined a number of commitments and actions to address racism within the sector. There is a particular focus on implementing the One Vision One Voice Framework, which is a provincial (Ontario) framework to address racism and inequities and improve outcomes for Black and racialized children.
The National Collaborating Centres for Public Health produce information to help public health professionals improve their response to health inequities and more.
The National Collaborating Centre for Indigenous Health (NCCIH) provides publications and a series of fact sheets on anti-Indigenous racism in Canada: This series of three fact sheets focuses on racism experienced by Indigenous peoples in Canada. The first fact sheet is on understanding racism, the second deals with Indigenous experiences with racism and its impacts and the third is on policies, programs and strategies to address anti-Indigenous racism.
The National Collaborating Centre for Determinants of Health (NCCDH) provides publications, webinars and other information on racial equity, anti-racism, and anti-Black racism.
Allyship
Allyship is defined as “an active, consistent, and arduous practice of unlearning and re-evaluating, in which a person in a position of privilege and power seeks to operate in solidarity with a marginalized group” (Anti-oppression Network[AON], n.d.).
It is a lifelong process of building relationships based on trust, consistency, and accountability with marginalized individuals and/or groups of people (AON, n.d.).
Allyship is not self-defined and it is not an identity. Instead, those being supported by allies must recognize the work and efforts (AON, n.d.).
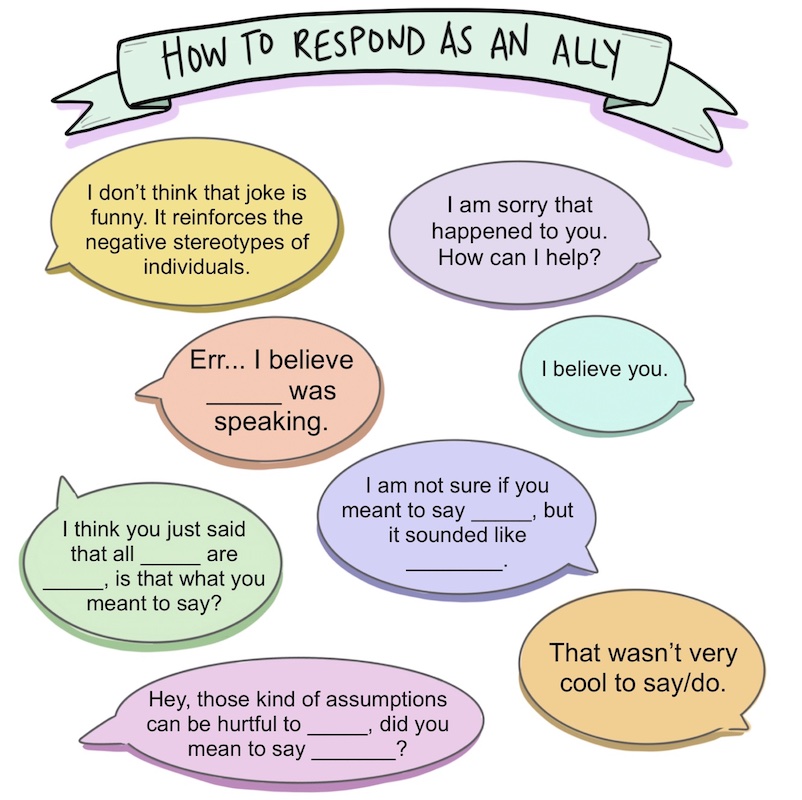
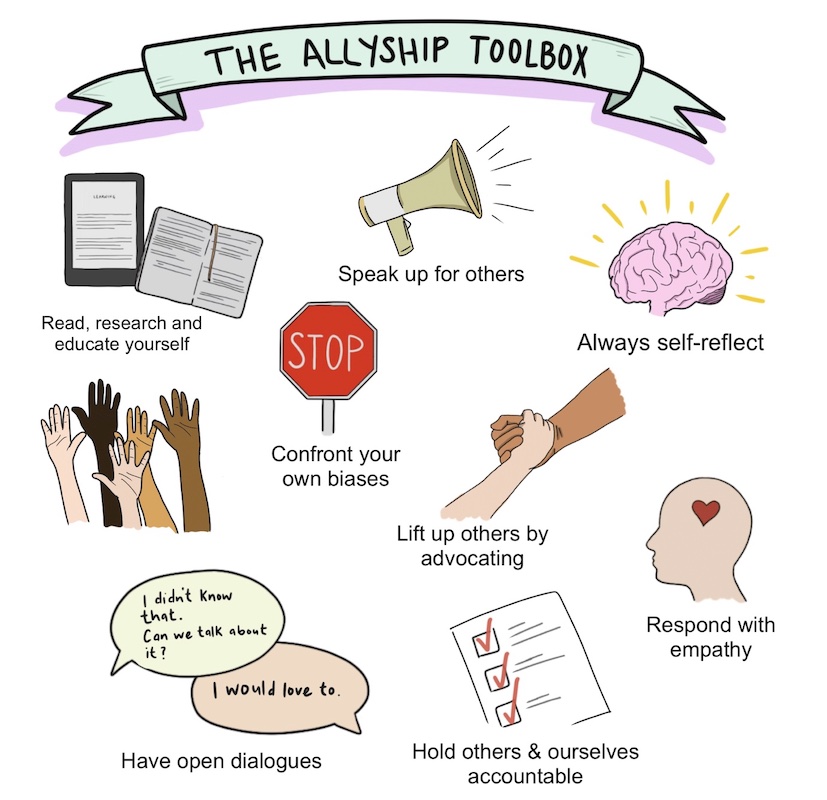
The Hospital for Sick Children in Toronto developed tools alongside a workshop, to teach health providers more about allyship. An article about that workshop, as well as two infographics from it, are featured below.
Sociodemographic data
As previously highlighted in the course, addressing disparities in different communities requires individualized health promotion and illness prevention and treatment for each group (Bates et al., 2017). Sociodemographic data can help organizations understand the disparities, barriers and facilitators to equity.
Collecting sociodemographic data about health service users is crucial for selecting, implementing and evaluating effective, equitable approaches and interventions. More specifically, sociodemographic data “enables system accountability, tracking of geographical and demographic data patterns (and) tracking of pathways of health outcomes, disease patterns and program interventions” (Bates et al., 2017). In addition, the insufficiency or incompleteness of data prevents full understanding of the challenges faced by communities and could lead to deceptive outcomes (Bates et al., 2017).
Current sources of data include the census, sample surveys (e.g., Canadian Community Health Survey) and administrative data collected when clients use services.
This manual, by the World Health Organization, is a practical reference for identifying and monitoring health inequalities through data collection and analysis.
The Canadian Institute for Health Information’s Measuring Health Inequalities: A Toolkit is designed to assist with measuring and reporting on health inequalities with stratification of sociodemographic data.
The Knowledge Institute on Child and Youth Mental Health Addictions resource hub provides information on how to use race-based data to advance mental health equity.